Description
Intensive Care Unit (ICU) patients are often kept overnight, with average stays lasting 4 days ± 7.2 days. Common complications that lead to hospital stays include accidents, serious short term-conditions (i.e. heart attack/stroke), serious infections (i.e. sepsis), & major surgeries . Poor sleep is associated with these circumstances. ICU patients commonly self-report an average of 4.0 ± 1.7 hours of sleep per night, compared to an at-home average of 7 ± 2.2 hours of sleep per night . Most environmental complaints observed from our interviews revolved around pain, anxiety, light, noise, environmental movement, & medication dosing. Common interventions reported included medication, closing patient doors, turning off lights, & limiting movement within patient rooms. However, studies have yet to establish conclusive relationships between non-medication-based interventions & increased sleep quality within hospital settings. Previous studies have also provided evidence of a decrease in patient stays, in 30-day readmission rates, and need for medicinal interventions with patients also reporting an increase in positive mental health rating as sleep quality improved within hospitals.
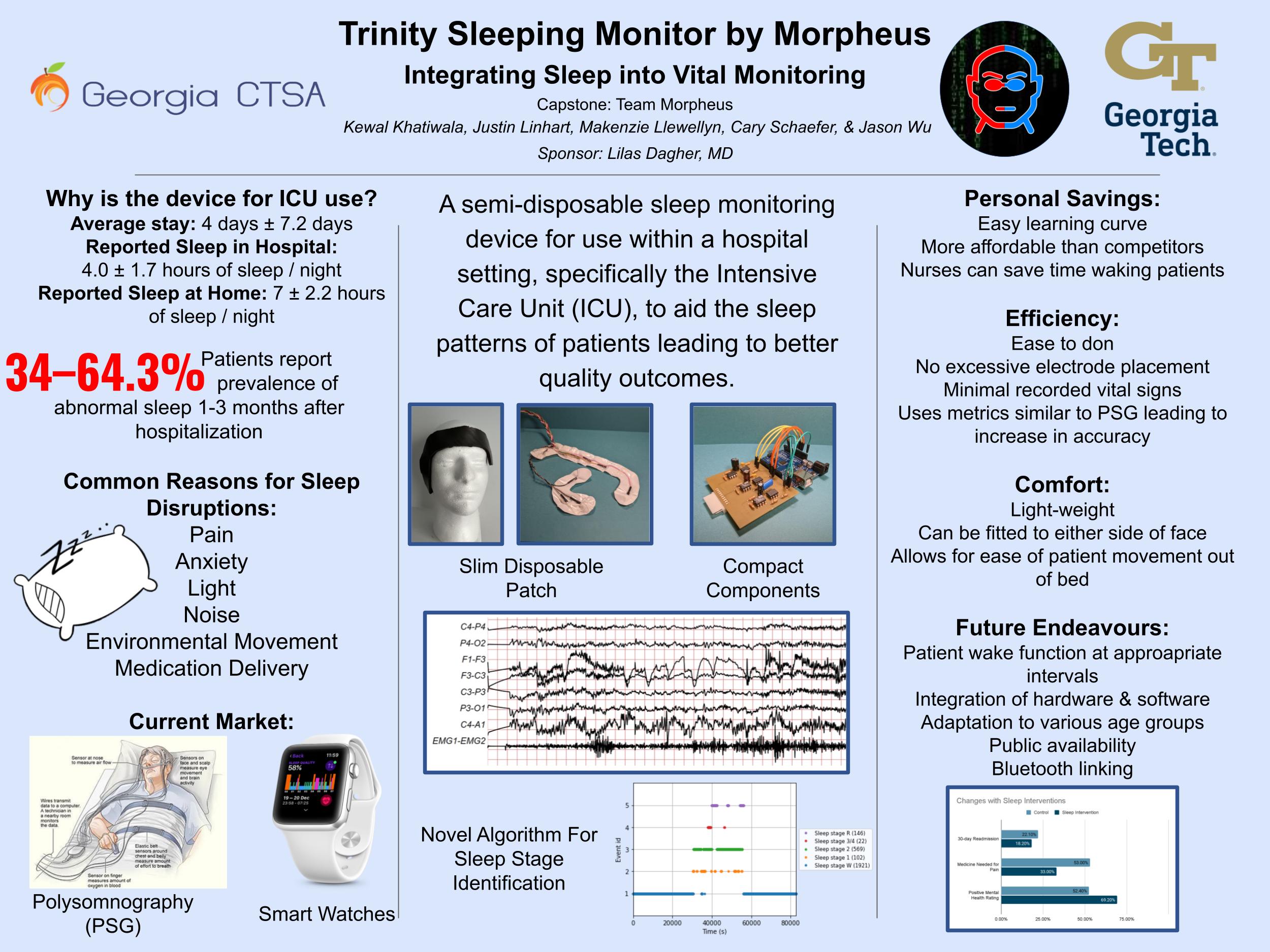
The aim of our device is to limit disruptions during patient REM cycles within the ICU setting, where our sponsor, Lilas Dagher, is currently fulfilling her residence at Emory. Our device is a semi-disposable sleep monitor for use within the ICU to aid the sleep patterns of patients leading to better quality outcomes and limit hospital stays. To achieve this our device can be broken down into three different components: a slim disposable patch, a component box housing circuitry, and a novel algorithm for sleep stage identification. As there are no current standards for sleep monitoring within a hospital setting, we based our device around sleep studies, or polysomnography (PSG). The PSG system is composed of a multitude of various sensors and electrodes. In order to simplify our device we chose to have our device only monitor brain waves via electroencephalogram (EEG), rapid eye movement via electrooculography (EOG), and middle ear muscle activity (MEMA) via electromyography (EMG). Our novel algorithm uses these three signals to determine if the patient is in REM sleep or non-REM sleep and provides feedback to the nurse. It also allows the nurse to set a schedule for waking the patient for medication delivery after the patient's REM cycle is complete. Having daily accessible sleep cycle recording will also aid in the the assessment of the patient’s clinical progress as disturbed sleep cycles are associated with worsening outcomes. Preliminary data has indicated the effectiveness of the Morpheus Sleep Monitor by verifying the signals collected and running simulated data through our code.